Effective: 07-11-22
Supersedes: 07-01-19 (start of contract)
Purpose: Provide guidance on the requirements of Brewster Ambulance Service in regards to the City of Framingham 911 Contract and Standard Operating Procedures.
Policy: Brewster Ambulance Service will provide both Advanced Life Support and Basic Life Support service to the City of Framingham 24 hours a day, 7 days a week.
Procedure:
The Framingham Fire Department shall be notified of all emergency responses within the Framingham City limits, as well as Mutual Aid requests.
Requirements :
Primary 24/7/365 ALS coverage
Coverage and Back Up Coverage:
ALS preferential when available, BLS ASAP when all dedicated vehicles are engaged in an emergency response or in patient care.
Coverage units will be dispatched by Brewster Ambulance Communications and should sign on with Fire Alarm who will assign coverage. Primary Units will post at Framingham Fire Stations as referenced below, unless directed otherwise by Framingham Fire Department. Back Up Units will post at MWMC Framingham or 280 Irving St.
A1 – FFD Station 5 – 520 Concord Street.
A2 – Station 8 – 7 Main Street.
A3 – FFD Station 3 HQ – 10 Loring Drive.
A4 – FFD Station 7 – 791 Water Street.
A5 – FFD Station 2 – 75 A Street.
FS3 – Brewster Framingham – 280 Irving Street
Units will communicate status updates to both Brewster Communications and Framingham
Fire until at destination.
Units will clear with both Brewster Communications and Framingham Fire Alarm via MDT/radio 24/7.
Dispatch Procedure:
Regardless of how the call is received by Framingham Fire Alarm (Framingham Fire phone lines, Framingham PD, Brewster EMD, walk-in, etc.) Framingham Fire Alarm will dispatch all appropriate units based on the district that the response is needed or the closest appropriate unit. All updates to patient care will be passed to responding units through Framingham Fire Alarm on their recorded radio frequencies.
Framingham Fire Alarm dispatches the appropriate unit via Radio and MDT.
If the call originates from a Brewster Communications line, Brewster Ambulance Service must notify Framingham Fire via telephone within two (2) minutes.
Further radio traffic will be over both Framingham Fire channel and Brewster Ambulance Service radio, including assignment of covering vehicles.
Unit Capabilities:
FS3
FS3 will be licensed through the Commonwealth of Massachusetts as a Class V Advanced Life Support ambulance staffed with ONE (1) Paramedic and a full complement of ALS equipment and pharmacology identified by Massachusetts OEMS.
FS3 will serve as a 24/7, dedicated ALS Supervisor for the City of Framingham. FS3 is not an IFT resource. FS3 is able to respond outside of the City of Framingham in the Metrowest area if a supervisor is needed at a serious incident (Brewster-involved MVC, patient injury, stretcher-tip, etc.) with approval of C2, the on-duty FFD Shift Commander. If it is determined that the incident will be extended (60 minutes or longer), another Brewster supervisor or manager will respond to assume control of the incident and relieve FS3 to their primary responsibilities in Framingham.
A1-A5
A1-A5 will be licensed through the Commonwealth of Massachusetts as a Class 1 Advanced Life Support ambulance staffed with ONE (1) Paramedic and ONE (1) Emergency Medical Technician (or higher) with a full complement of ALS equipment and pharmacology identified by Massachusetts OEMS. All units will have carbon monoxide monitoring capabilities, Stryker Stair Chairs, power stretchers, and LUCAS Device.
Dispatch Criteria:
A1-A5 will remain the primary response vehicles for incoming EMS responses. In the event the following patient conditions are noted through the call taking or EMD, FS3 will be dispatched to assist PB units with patient care and or transport. If FS3 is unavailable (i.e. already committed to another incident), a second ALS ambulance will be dispatched to assist with patient care and transport. The initial ambulance may cancel additional units after making an initial assessment of the patient on scene.
Those conditions include:
· Unresponsive or unconscious patient
· Cardiac Arrest
· Party Not Breathing
· Childbirth Emergencies
· Hemodynamic instability
· Anaphylactic Shock
· Patient Entrapment
· Pediatric Trauma
· Mechanical Ventilators
· Any Vasoactive Medications
· Multiple Medication Infusions
Interfacility Transport:
A1-A5 will support Heart Team activations and STAT transfer requests from MetroWest Medical Center for patients in urgent need of services or interventions unavailable at MWMC.
The Metrowest Medical Center Framingham Medical Director has identified the following conditions for STAT transfer requests for which they require immediate response to the hospital:
· AAA with no vascular surgery available
· Epidural with no neurosurgery available
· Symptomatic/unstable Intracranial hemorrhage or subdural hematoma with no neurosurgery available
· Type A aortic dissection
· Unstable patients with complex operative surgical conditions requiring tertiary care surgical services
· Septic infected obstructed ureteral stones with no urology available
· Vision threatening eye trauma
· Amputations with potential for salvage
· Potential status seizures with no EEG monitoring available
· Unstable pediatric patients needing a PICU
· Unstable trauma patients
· Unstable lower GI bleed requiring Interventional Radiology
This list is not all inclusive and may be modified as appropriate by FS3.
Procedure for STAT Transfer;
1. MWMC or Brewster will notify FS3
2. FS3 will contact and discuss recommendations for ambulance selection with Framingham Fire Shift Commander
3. FS3 will notify Fire Alarm of the ambulance selection
4. Framingham Fire Alarm will dispatch the appropriate unit and treat as a normal incident in CAD.
5. FS3 will send details of the incident to the Framingham Fire Shift Commander via email.
6. Framingham Fire Shift Commander will complete Fire Report including details for the reason of the STAT transfer in the narrative.
Posting:
A1 –Station 5 – 520 Concord Street.
A2 –Station 8 – 7 Main Streeet.
A3 –Station 3 HQ – 10 Loring Drive.
A4 –Station 7 – 789 Water Street.
A5 –Station 2 – 75 A Street.
FS3 –Brewster Framingham – 280 Irving Street. and Roaming
Dispatcher must honor all EMS mutual aid requests from the City of Framingham.
Special Events:
Brewster Ambulance Service will work in conjunction with the Framingham Fire/Police Department to ensure an adequate EMS plan and response for events.
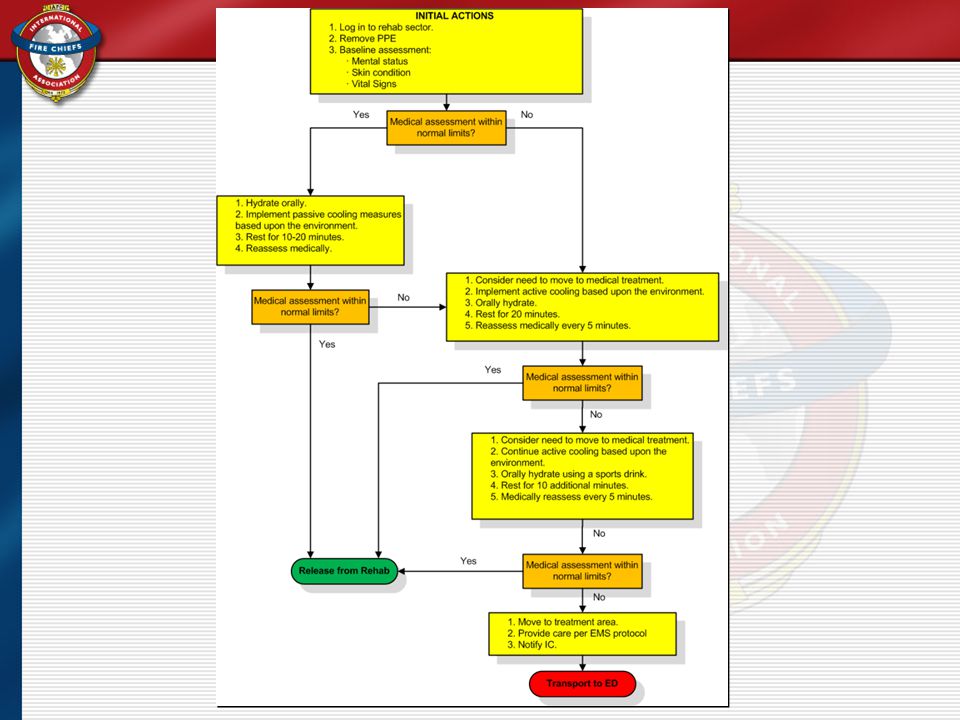
EMS Principles for Rehab at Emergency Incidents
EMS personnel may be designated by the Incident Commander (IC) at the scene of an emergency or training exercise to perform the function as rehab providers to assure the safety and well-being of the emergency responders, and the overall integrity of the operation. The need for establishing a Rehab Sector shall be based upon the duration, complexity, intensity of the incident and the climatic conditions, but shall not be the sole criteria for establishing Rehab.
The IC may establish a Rehab Manager as his/her designee. The Rehab Manager shall assure that all resources necessary to operate the Rehab Sector are communicated to the Logistics Officer or IC. The Rehab sector shall provide rest for the emergency responders. Adequate resources for re-hydration, cooling/warming, medical screening, and accountability shall be available. Multiple Rehab locations may be necessary based on the size of the incident. Each Rehab area shall have its own manager and identification, i.e.: Rehab 1, Rehab 2.
The Rehab Manager shall assure that adequate EMS staffing (paramedic level preferred) shall be available for responder screening and medical treatment if necessary. A dedicated ambulance (ALS level) shall be assigned to the Rehab Sector for the duration of the incident. Easy access by EMS vehicles to the Rehab Sector shall be maintained at all times.
All emergency responders directed to the Rehab Sector by the IC shall be screened according to local protocol, and the attached “Rehab Flow Chart”. Any emergency responder who presents at the Rehab Sector with an acute medical condition shall be considered a patient under the definition of 105 CMR 170.020 and shall be treated in accordance with the appropriate Statewide Treatment Protocol. The Rehab Manager shall be responsible for tracking all responders entering and exiting the Rehab area, or who are transported from Rehab to a medical facility.
MCI Activation:
An MCI declaration signifies that an incident has occurred in which the number of casualties is expected to overwhelm the EMS system. Any of the following individuals or organizations can declare an MCI: the public safety agency in charge of overall incident command, first arriving EMT on scene with an emergency vehicle, hospitals, CMED, regional council staff.
Once an MCI has been declared, request additional EMS resources and notify CMED so that they may notify hospitals of the type of incident and the expected number of casualties. When notifying CMED, use the acronym METHANE to provide an accurate scene size up.
Major incident declaration
Exact location of the incident, staging area if applicable
Type of incident; the nature of the incident, including how many vehicles, buildings etc. involved
Hazards; both present and potential
Access; best route for emergency services to access the site, or obstructions and bottlenecks to avoid
Numbers; of casualties, dead and injured on scene
Emergency services; which services are already on scene and which are still required (MCI trailer, Regional EMS Council staff, Task Force, etc.)
Levels:
Level 1: 1-10 potential victims
Level 2: 11-30 potential victims
Level 3: 31-50 potential victims
Level 4: 51-200 potential victims
Level 5: Greater than 200 victims
Level 6: Long-Term Operational period(s)
START TRIAGE
Primary Triage: First contact, assign triage category, ~30 seconds per patient
Secondary Triage: ongoing process that occurs after the patient has been moved to a treatment or staging area and is awaiting transport
Triage Categories:
Red: Immediate transport, critical patients
Yellow: Delayed, serious patient that can wait until all reds have been transported
Green: Hold, ambulatory, minor injuries
Black: Deceased
Procedure:
Start where you stand, and proceed in either a clockwise or counterclockwise direction until all patients have been assigned a triage category
First, identify the uninjured or “walking wounded”
Move them to a casualty collection point or have them assist you in controlling bleeding or maintaining airways.
Proceed to the victims that are not ambulatory:
Respirations:
None, attempt to open the airway, still no breathing tag BLACK
Respirations >30/min or <10/min, tag RED
Respirations between 10-30/ min, proceed to Step 2
Perfusion: check radial pulse or capillary refill
If cap refill >2 sec or no radial pulse, tag RED
If cap refill <2 and has a radial pulse tag YELLOW
If severe bleeding, apply tourniquet or bandage and place in recovery position
Mental Status:
Altered mental status or inability to follow commands, tag RED
If patient is unconscious, tag RED
If patient is able to follow commands, tag YELLOW
Establish contact with the Medical Branch Director and determine the areas to be used for triage and for ambulance staging
Move victims to patient treatment area
Upon completion of START triaging, assist with first aid in the patient treatment area
Assist with rescue, stabilization, fire control, hazard reduction, treatment and litter bearing as requested
Assist with loading of ambulances
Assist with establishment of morgue, if directed by Coroner
Additional Services / Equipment:
Brewster Ambulance Service will provide the following Vehicles and Medical equipment to further enhance the EMS response for the town:
· FS3 - ALS SUV
· Lucas Chest compression devices (A1-5)
· Stryker Stair Chair (A1-5)
· Cyanokits for cyanide toxicity (FS3)
· CO monitoring (all primary units)
· BLS Albuterol administration
· Selective spinal assessment
· ALS Cardiocerebral resuscitation
· Needle Cricothyrotomy
· Transexamic acid (Trauma)
· BLS use of glucometer
· Mobile Integrated Health (MIH in conjunction with MWMC Framingham)
Framingham EMS Fire Incident Response
Deputy Chief/Officer In Charge (OIC)
Working Fire/First Alarm
FS3
i. Establish Staging Area for Transporting Units
ii. Establish Medical IC at OIC’s discretion
First Transporting Unit on scene (A1-5)
i. Obtain H20 from station for rehab
ii. Create Rehab for Firefighters
iii. Post at Staging Area to standby for needed transports
Second Alarm
FS3
i. Establish Triage Area for Medical Patients at OICs Discretion
ii. Coordinate incoming units to Staging Area and Rehab
Second Transporting Unit
i. Pick up and Supply additional Rehab Resources as needed
ii. Standby at Staging Area or Rehab per FS3/OIC
Third Alarm
**FFD Contacts MDFS Rehab**
FS3
i. Maintain Triage and Staging Area for transporting units per OIC
Transporting Units
ii. Pick up and Supply additional Rehab Resources as needed
iii. Standby at Staging Area or Triage per FS3/OIC